
Introduction
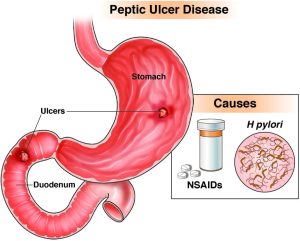
A peptic ulcer is characterized by the erosion or breakage of the mucous membrane or tissues within the digestive tract, which are regularly exposed to gastric juices containing hydrochloric acid (HCl) and pepsin. This erosion can extend through the muscle layer and even perforate the outer layers, leading to bleeding or perforation. Essentially, a peptic ulcer involves ulceration that affects the mucosal lining and deeper structures of the upper gastrointestinal tract and is caused by the corrosive action of gastric juices. It manifests as an excavation or hollowed-out area formed within the mucosal wall of the esophagus, stomach, or duodenum.
Epidemiology
- The highest frequency occurs between the ages of 40 and 60.
- The peak age for duodenal ulcers is between 30 and 60 years.
- Gastric ulcers typically peak in individuals aged 50 and older.
- The male-to-female ratio for duodenal ulcers is 2-3:1.
- For gastric ulcers, the male-to-female ratio is 1:1.
- Approximately 80% of peptic ulcer diseases (PUD) manifest as duodenal ulcers, while gastric ulcers account for about 15%
Common Sites:
- Lower esophagus
- Stomach
- Proximal portion of the duodenum
Types
Ulcers can be classified according to their degree and location.
Type according to degree:
- Peptic ulcers may be acute or chronic. Acute ulcers are often multiple and usually located in the fundus of the stomach. These ulcers are thought to be stress-related, superficial, and self-limiting. Occasionally, they penetrate a blood vessel, causing hemorrhages of varying degrees of severity.
- Chronic ulcers are more common than acute ulcers. These ulcers usually occur as a single lesion with margins that are thickened, hyperemic, and edematous. Chronic ulcers tend to recur frequently, causing extensive scarring.
Type according to location:
- Esophageal ulcers: These ulcers affect the lower portion of the esophagus and are usually due to a weaker esophageal sphincter, which allows gastric contents to escape into the esophagus.
- Gastric ulcers: These occur in the stomach, mainly in the lesser and greater curvatures and pyloric antrum. The occurrence is due to the defective ability of the stomach to heal faster.
- Duodenal ulcers: These are the commonest and are seen in the first portion of the duodenum. Ulcers result from the high secretion of hydrochloric acid.
Etiology
The erosion of the gastric mucosa is caused by the digestive action of hydrochloric acid and pepsin, although the exact cause is not fully understood. However, several factors precipitate the occurrence of peptic ulcers:
- The gram-negative bacteria Helicobacter pylori, present in 70% of patients with gastric ulcers and 95% of patients with duodenal ulcers, has been associated with peptic ulcers.
- Emotional factors: Emotional tension, anxiety, frustration, and stress may cause an imbalance in the autonomic nervous system, resulting in increased vagal stimulation of gastric secretion.
- Inflammation: Gastritis and trauma to the mucosa reduce the resistance of the membrane to digestion. Cell destruction is accelerated, and cell reproduction, which normally renews the superficial layers quickly, may be retarded.
- Hereditary factors: gastric ulcers are common in people with type A blood, while duodenal ulcers are common in people with type O blood. Duodenal ulcers are three times more common in first-degree relatives of duodenal ulcer patients than in the general population.
- Trauma and serious illness: Critical illnesses, especially those characterized by hypotension or respiratory insufficiency, may complicate peptic ulcers. Conditions such as severe burns, shock, etc., may lead to peptic ulceration.
- Prolonged use of irritants: Certain drugs, including non-steroidal anti-inflammatory drugs (NSAIDs), may predispose to peptic ulcer disease (e.g., acetylsalicylic acid, adrenal steroids, indomethacin, and phenylbutazone). Alcohol inhibits prostaglandin secretion. Nicotine in cigarette smoking inhibits pancreatic secretion of bicarbonate; it also may accelerate the emptying of gastric acid into the duodenum and promote mucosal breakdown.
- Bile Reflux: The reflux of bile and pancreatic enzymes into the stomach due to an incompetent pyloric sphincter may lead to a gastric ulcer. The bile salts damage the gastric mucosa, predisposing it to ulceration.
- Normal aging may also wear down the pyloric sphincter, which in turn permits the reflux of bile into the stomach.
- Zollinger Ellison Syndrome: A condition characterized by excessive production of hydrochloric acid, which erodes the gastric mucosa.
Epidemiology
Duodenal ulcers are very common, occurring 2–3 times more frequently than gastric ulcer disease.
Pathophysiology
Ulceration occurs due to a decrease in the resistance of the gastric mucosa to pepsin and acid injury. After the ingestion of food, acetylcholine, gastrin, and histamine bind to specific receptors and stimulate the parietal cells in the fundus of the stomach to secrete gastric acid. The parietal cells, with the assistance of H+ and K+ ATPases, transport the HCL to the stomach lumen. Meanwhile, the chief cells in the stomach secrete pepsinogen, which converts to pepsin in the presence of HCL to break down food.
Duodenal cells in the epithelium secrete a mucus barrier to protect the lining of the gastric-duodenal area. This mucus barrier dilutes the secretion of acid and provides a protective coating against acid action. Peptic ulcers may develop when the secretory output of hydrochloric acid exceeds that of pepsin, thereby eroding the gastric mucosa membrane due to inadequate defense secretion of mucus to neutralize the imbalance, thereby promoting ulcer development.
Signs and symptoms
Signs and symptoms of peptic ulcers include:
- Epigastric pain: gnawing or burning pain in the upper abdomen, often related to food intake and radiating to the back due to erosion of the mucosal lining.
- Heartburn (pyrosis): A burning sensation experienced in some patients due to excessive acid presence in the esophagus and stomach.
- Vomiting: Occurs due to severe pain and may also be caused by obstruction resulting from muscular spasms of the pylorus.
- Weight loss is especially common in individuals with gastric ulcers.
- Dyspepsia: Symptoms include belching, bloating, distention, and intolerance to fatty foods.
- Chest discomfort
- Anorexia: loss of appetite.
- Hematemesis, or melena, results from gastrointestinal bleeding from eroded small blood vessels. Melena stool, characterized by black, tarry stool, is more common in duodenal ulcers.
- Constipation: Occurs due to inadequate intake of fluids and fiber-rich foods.
Characteristic differences between gastric ulcers and duodenal ulcers:
Location of the Lesion:
- Gastric ulcers are predominantly found in the antrum of the stomach, as well as in the body and fundus.
- Duodenal Ulcers: typically occur in the first 2cm of the duodenum.
Lesion Characteristics:
- Gastric Ulcers: superficial lesions with smooth margins, often round, oval, or cone-shaped.
- Duodenal Ulcers: Penetrating lesions associated with deformity of the duodenum from the healing of previous ulcers.
Gastric Secretion:
- Gastric Ulcers: normal to decreased secretion.
- Duodenal Ulcers: increased secretion.
Incidence and Peak Age:
- Gastric Ulcers: Higher incidence in women; peak age typically between 50 and 60 years; more common in people of lower socioeconomic status.
- Duodenal Ulcers: higher incidence in men but also prevalent in post-menopausal women; peak age typically between 35 and 45 years.
Associated Factors:
- Gastric Ulcers: are associated with an incompetent pyloric sphincter and bile reflux.
- Duodenal Ulcers: are associated with other diseases such as pancreatic disease and Zollinger-Ellison syndrome.
Clinical Manifestations:
- Gastric Ulcers: Burning or gaseous pressure in the high left epigastric region, pain occurs 1-2 hours after meals and is aggravated by food, weight loss, and hematemesis may occur.
- Duodenal Ulcers: Burning and crampy pain across the mid-epigastrium and upper abdomen, pain occurs 2-4 hours after meals but is relieved with food, weight may be normal or the patient may gain more weight, melena may occur.
Blood Group:
- No significant difference was observed.
- Duodenal Ulcers: common in blood group O.
Cancerous Tendencies:
- Gastric Ulcers: More common to develop cancer.
- Duodenal Ulcers: Less common to develop cancer.
Diagnosis:
History Taking:
- Assess abdominal pain, including location, timing, severity, associated symptoms, and precipitating factors.
Physical Assessment:
- Carefully examine and palpate the abdomen, focusing on pain, typically present in the upper epigastrium, left of the midline.
Endoscopy (Esophagogastroduodenoscopy):
- Visualize and identify inflammatory changes, ulcers, and lesions in the upper gastrointestinal tract, including the duodenal mucosa.
Special Radiology:
- Perform a barium swallow and barium meal to visualize the ulcer after the patient has ingested barium sulfate.
Stool Examination:
- Detect the presence of blood (occult or fresh) in the stool, which may indicate bleeding from the gastrointestinal tract.
Biopsy:
- Conduct a biopsy for gastric ulcers to determine the benign or malignant status of the lesion.
Gastric Analysis:
- Aid in differentiating gastric ulcers from gastric cancer by analyzing gastric secretions.
Exfoliative Cytology:
- Examine secretions and cells brushed or scraped from the mucous membranes to further aid in diagnosis.
Drug Therapy Objectives:
- Provide pain relief.
- Eradicate the H. pylori infection.
- Promote ulcer healing by reducing gastric secretions and protecting the mucosa from further damage.
- Prevent the recurrence of ulcers.
Eradication Therapy
First-Line Therapy:
A recommended regimen for eradicating Helicobacter pylori in patients with gastric and duodenal ulcers is the use of a proton pump inhibitor (PPI) in combination with two antibiotics, such as Omeprazole, clarithromycin, and metronidazole.
Omeprazole:
- Dosage: 20mg orally twice daily for 4 to 8 weeks.
- Action: It inhibits the activity of the acid pump and binds to hydrogen-potassium adenosine triphosphatase to block the formation of gastric acid.
- Side Effects: headache, hallucinations, dizziness, diarrhea, abdominal pain, nausea, vomiting, constipation.
- Nursing Implications: Caution the patient not to perform hazardous activities if dizziness occurs; instruct the patient to swallow capsules whole and not to open or crush them.
Amoxicillin:
- Dosage: 500mg three times daily orally.
- Action: Blocks protein synthesis.
- Side Effects: Nausea, vomiting, diarrhea, abdominal pain, or discomfort.
- Nursing Implications: Use cautiously in patients with hepatic or renal impairment; obtain a urine specimen for culture and sensitivity tests before the first dose. Begin therapy pending results; monitor the patient for superinfection.
Metronidazole:
- Dosage: 400–500 mg orally three times daily.
- Side Effects: metallic taste, nausea, and vomiting.
- Nursing Implications: Instruct the patient to take the drug with food to minimize gastrointestinal discomfort.
Second-Line Therapy:
In cases where first-line therapy fails, a second-line regimen may be considered. This regimen typically includes a proton pump inhibitor along with bismuth, metronidazole, and tetracycline.
Bismuth:
- Dosage: 120mg four times daily.
- Action: Provides a protective coating to the gastrointestinal tract.
- Side Effects: May cause darkening of the tongue and stools.
- Nursing Implications: Monitor for signs of gastrointestinal upset and dark stools.
Metronidazole:
- Dosage: 400mg twice daily.
- Side Effects: metallic taste, nausea, and vomiting.
- Nursing Implications: Administer food to reduce gastrointestinal side effects.
Tetracycline:
- Dosage: 500mg twice daily.
- Action: inhibits bacterial protein synthesis.
- Side Effects: photosensitivity, gastrointestinal upset, tooth discoloration (avoid use in children).
- Nursing Implications: Advise patients to avoid prolonged exposure to sunlight and use sun protection measures. Monitor for gastrointestinal side effects and tooth discoloration.
Other Drugs
- Antacids:
- Mechanism: Antacids work by neutralizing gastric acid, thereby decreasing acidity in the stomach. They do not influence ulcer healing or prevent recurrence. Antacids aim to raise the pH in the stomach to around 3.0–3.5. They are typically taken after meals.
- Examples: aluminum hydroxide, magnesium trisilicate.
- Histamine Receptor Antagonists:
- Mechanism: Histamine receptor antagonists block the action of histamine, which stimulates acid secretion in the stomach. They are effective in managing ulcer disease by inhibiting acid secretion. Examples include Ranitidine (150mg twice daily) or Cimetidine (400mg twice daily for 4-6 weeks).
- Mucosal Barrier Fortifiers:
- Mechanism: Mucosal barrier fortifiers, such as sucralfate, stimulate mucus production and enhance ulcer healing. They form a protective barrier by adhering to the ulcer surface, preventing further damage to the mucosa. Sucralfate is typically administered as 1g orally four times daily or 2g twice daily, 1 hour before meals and at bedtime. It should not be administered within 30 minutes of antacids or other drugs.
- Anticholinergic Drugs:
- Mechanism: Anticholinergic drugs, like propantheline, are less commonly used compared to histamine receptor antagonists. They reduce gastric motility and secretion by decreasing vagal stimulation. This delay in gastric emptying time may promote ulcer healing and provide pain relief. However, they are not used in cases of bleeding or pyloric obstruction.
Nursing Management
Aims
- Alleviating Symptoms and Promoting Healing
- Reducing Anxiety
- Maintaining Nutritional Requirements
- Providing Education about Disease and Management
- Preventing Complications
Hospitalization Considerations:
- Hospitalization may not always be necessary
- If adherence to treatment is challenging or home environment is not conducive, hospitalization may be required
- The duration of hospitalization depends on symptom relief and patient understanding of treatment plan
Creating a Supportive Environment
- Promoting Rest: Ensure the environment supports both mental and physical rest. Nurse the patient in a quiet setting to minimize disturbances and promote relaxation, especially since patients with peptic ulcers experience severe pain.
- Ventilation: Ensure the environment is well-ventilated to enhance comfort and prevent feelings of stuffiness or discomfort.
- Stress Reduction: Remove stressful stimuli from the environment as much as possible. Stress can increase vagal activity, exacerbating the symptoms of peptic ulcers. Creating a calm and peaceful environment can help alleviate stress and promote healing.
- Comfort: Provide amenities that contribute to the patient’s comfort, such as adjusting the room temperature to a comfortable level, providing soft bedding, and ensuring adequate lighting.
- Safety: Ensure the environment is safe and free from hazards that could potentially harm the patient. Keep walkways clear, and ensure that any equipment or furniture is properly secured to prevent accidents.
- Privacy: Respect the patient’s privacy by maintaining confidentiality and providing them with a sense of personal space. This can contribute to their overall sense of well-being and comfort during their stay.
Rest
Rest, both mental and physical, plays a crucial role in reducing gastric activity and promoting healing in individuals with peptic ulcers. While a brief period of bed rest is essential, patients may also be encouraged to remain ambulatory with some restrictions on activity and an increase in rest hours. In severe cases, it may be necessary for patients to take time away from work, although for some, the anxiety caused by financial strain or disruption to their routine may outweigh the benefits of rest.
Creating a quiet and pleasant environment is paramount, as is ensuring physical comfort and providing undisturbed rest periods. Visitors who may evoke unpleasant feelings should be avoided, and diversion therapy can help alleviate anxiety. Nurses should listen attentively to patients, encouraging them to develop coping mechanisms for stressful situations that exacerbate symptoms. Providing perspective and offering constructive suggestions can help patients manage their anxiety levels.
In some cases, a sedative or tranquilizer may be prescribed to promote relaxation. It’s important to discourage visitors who may agitate the patient until their condition improves, allowing them the peace and tranquility necessary for healing.
Pain Relief
Assessment of the patient’s pain is essential, involving both verbal communication and observation of non-verbal cues such as grimacing or rubbing the affected area. Administer prescribed medications like Panadol to alleviate pain and enhance comfort, along with other medications aimed at promoting ulcer healing. Additionally, advise the patient to avoid highly spiced foods, as they can exacerbate pain and hinder the healing process. Providing diversional therapy, such as reading books or watching TV, can also help distract the patient from pain and promote relaxation.
Psychological Care
Effective psychological care plays a crucial role in the treatment of peptic ulcers, particularly due to their potential association with emotional factors. Begin by explaining the condition to the patient and their significant others in simple terms, covering aspects such as the disease process, affected parts of the body, associated signs and symptoms, causes, treatment options, and potential complications. This comprehensive explanation serves to impart knowledge and alleviate anxiety.
Encourage the significant others to refrain from alarming the patient with negative news or involving them in serious decision-making processes, as this could exacerbate stress. Instead, create an environment where the patient feels comfortable expressing their fears and concerns openly. Furthermore, involve the patient in developing plans for their care, fostering a sense of cooperation and empowerment in their treatment journey.
Observations
Continuous monitoring of the patient’s general condition is essential to gauging improvement or deterioration. Establish baseline data for vital signs, including pulse and blood pressure, which may indicate hemorrhage, as well as temperature and respirations, which can be affected by severe peptic ulcers.
Observe the patient for pain, noting its location and any exacerbating factors, such as specific foods. Monitor for vomiting episodes and examine the contents of the vomitus, as well as observe stool characteristics. Document and promptly report all findings to the responsible nurse.
Track the patient’s response to treatment and remain vigilant for any potential side effects of prescribed medications. Additionally, monitor for complications such as hemorrhage, which may manifest as dizziness, low blood pressure, a rapid, feeble pulse, or pyloric obstruction, indicated by vomiting of undigested food. Observe the patient’s dietary habits and assist in identifying foods that either alleviate or exacerbate pain, contributing to personalized care and symptom management.
Nutrition and Fluid Management
Nutrition plays a crucial role in the treatment of patients with peptic ulcers, as certain foods can either exacerbate or alleviate symptoms. Identify and avoid foods known to cause pain, as well as those that are highly seasoned or known to produce gas, as they can worsen the patient’s condition. Instead, provide a well-balanced diet rich in proteins to support ulcer healing and roughage to prevent constipation, a common issue.
Offer food in small, frequent portions to promote appetite and reduce the likelihood of vomiting. Encourage fluid intake, either orally or intravenously, depending on the patient’s condition, to prevent dehydration resulting from vomiting and to help neutralize hydrochloric acid in the stomach. This approach supports overall patient comfort and aids in symptom management.
Elimination Management
Monitor intake and output closely, recording measurements to prevent fluid overload. Offer a diet rich in roughage to facilitate bowel movements and prevent constipation, a common concern in patients with peptic ulcers. Regularly inspect stool and vomitus for signs of blood, and promptly inform the physician if any abnormalities are noted. Additionally, provide an emesis bowl to assist with vomiting episodes, ensuring patient comfort and cleanliness. These measures contribute to effective elimination management and overall patient well-being.
Exercises and Hygiene Management
Exercises: Initially, patients with peptic ulcers should be placed on total bed rest to prevent stress and excessive stimulation of the vagus nerve, which can increase hydrochloric acid production. As the patient’s condition improves, introduce gentle exercises gradually to prevent complications such as deep vein thrombosis associated with prolonged bed rest.
Hygiene: Provide assistance to patients with bathing to enhance comfort, promote blood circulation, and maintain cleanliness, thereby reducing the risk of infection. Perform oral care regularly to stimulate appetite, prevent halitosis (bad breath), and maintain oral hygiene. Ensure the timely changing of bed linens as needed to maintain cleanliness and prevent skin irritation. These measures contribute to overall patient comfort and well-being while minimizing the risk of complications associated with immobility and poor hygiene.
Patient Education
- Educate the patient about avoiding precipitating factors such as caffeinated drinks and alcohol ingestion, which can exacerbate symptoms.
- Assess the patient’s current knowledge of managing the condition to establish a baseline for further education.
- Determine the patient’s willingness and ability to learn, ensuring comprehension of the condition and its management.
- Assist the patient in identifying stressors and making modifications to daily routines to reduce stress-induced hypersecretion of gastric acid and pepsin.
- Discuss dietary plans and provide guidance on implementation both at home and in the workplace.
- Teach the patient to recognize warning signs and symptoms of recurrent ulcers or complications, and stress the importance of seeking early treatment.
- Explain the harmful effects of smoking, which directly irritates the gastric mucosa and can worsen symptoms.
- Provide a rationale for eliminating alcohol, spicy foods, coffee, tea, and cola from the diet, emphasizing their impact on ulcer symptoms.
- Offer written materials on the condition to reinforce understanding and provide additional resources for reference.
- Emphasize the importance of adhering to prescribed medication regimens and educate on the potential side effects of the drugs. Discourage the use of unprescribed drugs such as aspirin.
- Reinforce the need for regular follow-up appointments to monitor progress and adjust treatment as needed.
Complications
Hemorrhage: This is the most common complication associated with peptic ulcer disease, occurring when the ulcer erodes a blood vessel. Signs of hemorrhage include vomiting blood (hematemesis) and passing black, tarry stools (melena). In cases of massive bleeding, patients may experience weakness, apprehension, dizziness, and faintness, which can progress rapidly to prostration and loss of consciousness. Physical signs include pale, cold, and clammy skin, a rapid and thready pulse, and abnormally low blood pressure. Rapid respirations may indicate air hunger and hypoxemia. If a large blood vessel is eroded, signs and symptoms appear more rapidly, and collapse can occur quickly.
Perforation: Perforation is a serious and potentially life-threatening complication resulting from the progressive erosion of ulcers through the layers of the gastrointestinal wall, including the submucosal, muscular, and serous layers. When the serous membrane is breached, stomach or duodenal contents can leak into the peritoneal cavity, leading to generalized peritonitis due to chemical irritation and infection. Perforation is more common in duodenal ulcers and can occur even in individuals with no previous ulcer history.
Symptoms of perforation include sudden and severe abdominal pain starting in the mid-epigastric region and spreading throughout the abdomen. The patient may exhibit pallor, cold clammy skin, a rapid pulse, shallow, grunting respirations, and may experience nausea and vomiting. Upon examination, the abdomen becomes tender, rigid, and board-like. Patients may adopt a knee-chest position to alleviate tension on the abdominal muscles. Perforation can lead to complications such as bacterial septicemia, hypovolemic shock, and paralytic ileus, further complicating the patient’s condition and requiring prompt medical attention.
Peritonitis -can develop as a consequence of perforation into the peritoneal cavity. Gastric outlet obstruction occurs due to edema, inflammation, and fibrous scar formation. Symptoms include abdominal bloating, nausea, and vomiting. Persistent vomiting can lead to alkalosis due to the loss of acid gastric juice in vomit, resulting in hypokalemia from the loss of chloride ions.
Malignancy -may arise from the chronic ulceration-induced regeneration of epithelium. Penetration occurs when an ulcer on the posterior wall of the duodenum or stomach perforates into adjacent structures such as the pancreas, liver, or biliary tree. Patients may experience intensified and constant pain, possibly radiating to the back, which does not respond to antacids or food.
Read more: Medical-Surgical Nursing
Read more: Gastritis | Nursing Management
[…] Read more: Peptic ulcers | Nursing Management […]