
What is a hookworm?
Hookworm disease, also known as hookworm infection or ancylostomiasis, is a parasitic infection caused by hookworms. There are two main species of hookworms that infect humans: Ancylostoma duodenale and Necator americanus. These parasites primarily affect the small intestine of humans.
Hookworm infection poses a significant health burden, particularly in the developing regions of the tropics and subtropics, where it is a major cause of maternal and child morbidity. Susceptible children, when infected with hookworms, can experience intellectual, cognitive, and growth impairments. Additionally, maternal infection during pregnancy can lead to intrauterine growth retardation, prematurity, and low birth weight in newborns. While hookworm infection itself is seldom fatal, it can result in significant anemia, particularly in individuals with heavy worm burdens.
Epidemiology
It is currently estimated that between 576 and 740 million people worldwide are harboring hookworm infections. Among this population, approximately 80 million individuals suffer from severe manifestations of the disease.
Causes of Hookworm Infection
Species of Hookworms: Two species of hookworms commonly infect humans: Ancylostoma duodenale and Necator americanus.
Prevalence
- Necator americanus predominates in the Americas, Sub-Saharan Africa, Southeast Asia, China, and Indonesia.
- Ancylostoma duodenale predominates in the Middle East, North Africa, India, and previously in southern Europe.
Disease Presentation
- Hookworm infection leads to ankylostomiasis, also known as anchylostomiasis or helminthiasis.
- The disease occurs when hookworms, present in large numbers, feed voraciously on blood from the host’s intestinal walls, resulting in iron deficiency anemia.
Morphology of Ancylostoma duodenale Worms
- Ancylostoma duodenale worms appear greyish-white or pinkish, with the head slightly bent in relation to the rest of the body.
- They have well-developed mouths equipped with two pairs of teeth.
- Males typically measure about one centimeter in length and 0.5 millimeters in width, while females are often longer and more robust in size.
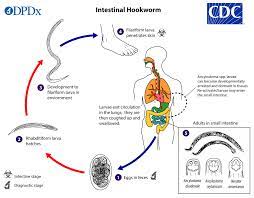
The life cycle of Hookworms
- Eggs in the Environment: The life cycle begins when adult female hookworms in the small intestine of the host produce eggs. These eggs are passed out through the host’s feces into the environment.
- Larval Development: In favorable conditions of warmth, moisture, and oxygen, the eggs hatch into larvae within the soil.
- Infective Larvae: The larvae molt twice to become infective larvae (L3 stage), which can penetrate the skin of the host, usually through bare feet, during contact with contaminated soil.
- Migration to the Small Intestine: Once penetrated, the larvae migrate through the bloodstream to the lungs, ascend the respiratory tract, are swallowed, and eventually reach the small intestine.
- Maturation into Adults: In the small intestine, the larvae mature into adult hookworms. They attach to the intestinal mucosa and begin feeding on the host’s blood.
- Egg Production: Adult female hookworms produce eggs, which are passed out in the host’s feces, completing the life cycle.
Life Cycle of N. americanus and A. duodenale in the Environment
- Eggs of N. americanus and A. duodenale are commonly found in warm, moist soil, where they undergo development until they hatch into first-stage larvae.
- These newly hatched larvae enter a feeding, non-infective stage known as the rhabditoform stage. During this stage, they feed on soil microbes.
- After a period of feeding, the larvae molt into second-stage larvae, which also remain in the rhabditoform stage. They continue to feed for approximately 7 days.
- Following this feeding period, the larvae undergo another molt, transitioning into the third-stage larvae.
- The third-stage larvae, known as the filariform stage, are the non-feeding infective form of the parasite. They are capable of penetrating the skin of the host to initiate infection.
Life Cycle In Man
- Larvae enter the lungs through the pulmonary capillaries and break out into the alveoli.
- They travel up the trachea and are coughed up and swallowed by the host.
- After ingestion, larvae are found in the small intestine, where they molt into the adult worm stage.
- The entire process, from skin penetration to adult development, takes about 5–9 weeks.
- Female adult worms release eggs (N. Americanus: about 9,000–10,000 eggs/day; A. duodenale: 25,000–30,000 eggs per day), which are passed in the feces of the human host.
- These eggs hatch in the environment within several days, initiating a new cycle.

The incubation period
The incubation period of hookworm infection can range from a few weeks to several months, and its duration largely depends on the severity of the infestation, determined by the number of hookworm parasites present in the individual.
In cases where the infection involves a high burden of parasites, symptoms may manifest more rapidly, leading to a shorter incubation period. Conversely, patients with lower levels of infestation tend to experience a more prolonged incubation period before symptoms become apparent.
Pathophysiology
Hookworm infection is typically considered asymptomatic, yet it poses significant danger due to its “silent and insidious” nature. While patients may initially experience general symptoms soon after infection, such as ground-itch, a common allergic reaction at the site of larval entry, particularly in N. americanus infections, there may be additional manifestations as the infection progresses.
- As the larvae break into the alveoli and ascend the trachea, symptoms like coughing and pneumonitis may arise.
- Upon reaching the small intestine and beginning maturation, infected individuals commonly suffer from diarrhea and gastrointestinal discomfort.
However, the true insidiousness of hookworm infection lies in chronic, heavy-intensity cases. Major morbidities stem from intestinal blood loss, iron deficiency anemia, and protein malnutrition. This results primarily from adult hookworms ingesting blood, rupturing red blood cells, and degrading hemoglobin in the host.
- Chronic blood loss can lead to physical manifestations like facial and peripheral edema, as well as eosinophilia and pica due to iron deficiency anemia.
- It’s widely recognized that children with chronic hookworm infection may experience growth retardation, intellectual impairment, and cognitive deficits due to the long-term effects of the parasite on their health.
Signs and Symptoms
- Gastrointestinal Inflammation: Symptoms in patients often arise due to inflammation in the gut caused by the feeding activity of hookworms.
- Nausea: Patients may experience feelings of nausea, particularly as a result of gut irritation.
- Abdominal Pain and Intermittent Diarrhea: Common symptoms include abdominal pain and sporadic episodes of diarrhea, which can be linked to the inflammatory response and damage caused by the parasites in the intestines.
- Progressive Anemia: In cases of prolonged infection, progressive anemia may develop due to chronic blood loss from the intestinal mucosa, leading to symptoms such as fatigue, weakness, and pallor.
- Capricious Appetite and Pica: Affected people may exhibit changes in appetite, ranging from unpredictability to the development of pica, a condition characterized by cravings for non-food items such as dirt or clay, often associated with nutritional deficiencies.
- Gastrointestinal Disturbances: Symptoms may include obstinate constipation followed by episodes of diarrhea, reflecting the disruptive effect of the parasites on normal bowel function.
- Cardiovascular Symptoms: Palpitations, a thready pulse, and coldness of the skin may occur, reflecting the impact of anemia on cardiovascular function.
- General Weakness and Fatigue: Individuals may experience overall fatigue and weakness due to the combined effects of anemia and systemic inflammation.
- Shortness of Breath: Anemia and reduced oxygen-carrying capacity in the blood may lead to symptoms of dyspnea or shortness of breath.
- Severe Complications: In severe cases, the infection may lead to complications such as dysentery, hemorrhages, and edema, potentially resulting in a fatal outcome if left untreated.
Medical Management
History
- Travel History: A nurse should ask about any recent travel to regions where hookworm infection is prevalent, particularly tropical and subtropical areas with poor sanitation.
- Exposure to Contaminated Environments: Ask about exposure to soil or water sources potentially contaminated with hookworm larvae.
- Symptomatology: Make sure that a nurse evaluates for symptoms such as abdominal pain, diarrhea, nausea, fatigue, weakness, shortness of breath, and changes in appetite.
- Medical History: Obtain information about any previous episodes of gastrointestinal disorders, anemia, or unexplained fatigue.
- Occupational and Living Conditions: Assess living conditions, including sanitation facilities, and inquire about occupations involving soil exposure.
Physical Examination
- General Appearance: Assess for signs of pallor, fatigue, and overall weakness, which may indicate anemia and the systemic effects of the infection.
- Skin Examination: Look for signs of ground-itch or dermatitis at potential sites of larval penetration, such as the feet.
- Abdominal Examination: Palpate the abdomen for tenderness, distention, or masses, and assess bowel sounds. Abdominal pain and tenderness may suggest gastrointestinal inflammation.
- Cardiovascular Examination: Check for any signs of tachycardia, palpitations, or hypotension, which may indicate anemia-related cardiovascular compromise.
- Respiratory Examination: Evaluate for signs of respiratory distress, cough, or abnormal breath sounds, which could indicate pulmonary involvement if larvae have migrated to the lungs.
- Nutritional Assessment: Look for signs of malnutrition, including muscle wasting, edema, and skin changes such as dryness or scaling.
- Neurological Examination: Assess cognitive function and look for signs of neurological deficits, particularly in children, as chronic hookworm infection can affect intellectual development.
Investigations
- Stool Examination: The microscopic examination of stool samples to check for the presence of hookworm eggs is the primary diagnostic test for confirming hookworm infection. Eggs can be detected using various techniques, such as direct smears, concentration methods (e.g., sedimentation or flotation), or fecal immunoassays.
- Complete Blood Count (CBC): A CBC will reveal signs of anemia, such as low hemoglobin and hematocrit levels, as well as microcytic or hypochromic red blood cells, which are suggestive of iron deficiency anemia commonly associated with hookworm infection.
- Peripheral Blood Smear: Examination of a peripheral blood smear will reveal characteristic changes associated with anemia, such as hypochromic red blood cells and increased numbers of reticulocytes.
- Serum Iron Studies: Measurement of serum iron, ferritin, and total iron-binding capacity (TIBC) can help assess iron status and confirm iron deficiency anemia.
- Stool Occult Blood Test: This test detects the presence of blood in stool samples, which may indicate intestinal bleeding caused by hookworm infection.
- Serological Tests: Serological assays, such as enzyme-linked immunosorbent assays (ELISA), can detect antibodies against hookworm antigens and may be useful for confirming infection, especially in cases where stool examination is inconclusive.
- Imaging Studies: In severe cases or when complications such as intestinal obstruction or perforation are suspected, imaging modalities such as abdominal ultrasound or computed tomography (CT) scans may be employed to assess the extent of gastrointestinal involvement.
- Endoscopic Evaluation: In cases of suspected gastrointestinal bleeding or inflammatory bowel disease-like symptoms, upper gastrointestinal endoscopy or colonoscopy may be performed to visualize the mucosa and obtain biopsy samples for histological examination.
Treatment
- Albendazole Efficacy: Albendazole is effective against hookworm infection, targeting both the intestinal stage and the larval stage while the parasite is still migrating under the skin. It works by disrupting the function of the parasite’s β-tubulin protein, inhibiting microtubule polymerization, and ultimately killing the adult worms.
- Iron Supplementation: In cases of anemia resulting from hookworm infection, iron supplementation is very important to alleviate the symptoms of iron deficiency anemia. However, as red blood cell levels are restored, deficiencies in other essential nutrients such as folic acid or vitamin B12 may arise. Then, supplementation with these nutrients may also be necessary to prevent further complications.
- Benzimidazoles (BZAs): The primary treatment for hookworm infection involves the use of benzimidazole anthelmintic medications, specifically albendazole and mebendazole. These drugs work by binding to the nematode’s β-tubulin, disrupting microtubule polymerization, and ultimately killing the adult worms.
- Alternative Treatments: In certain circumstances, alternative medications such as levamisole and pyrantel pamoate may be used. These drugs also target the nematode’s nervous system, leading to paralysis and the expulsion of the worms from the intestines.
- Treatment Duration: The duration of treatment typically ranges from 1 to 3 days, depending on the severity of the infection and the specific medication used. Repeat doses may be necessary in cases of persistent or recurrent infections.
- Mass Drug Administration (MDA): In regions where hookworm infection is endemic, mass drug administration programs may be implemented to control the spread of the disease. These programs involve the distribution of anthelmintic medications to entire communities at regular intervals to reduce the prevalence of infection.
- Monitoring and Follow-Up: After treatment, patients should be monitored for resolution of symptoms and signs of anemia. Follow-up stool examinations may also be performed to confirm clearance of the infection. Additionally, efforts to improve sanitation and hygiene practices are essential for preventing reinfection and controlling the spread of hookworm infection within communities.
Nursing Diagnosis
- Impaired Growth and Development
- Inadequate Nutrition
- Diarrhea
- Fatigue
- Risk for Fluid Volume Deficit
- Risk for Infection
- Lack of Knowledge
- Ineffective Breathing Pattern
Nursing Management
Aims
- Alleviate Symptoms: The primary aim is to alleviate symptoms associated with hookworm infection, including abdominal pain, diarrhea, anemia, and fatigue, through appropriate nursing interventions and supportive care.
- Prevent Transmission: Nurses strive to prevent the transmission of hookworm disease by educating patients and communities about proper sanitation and hygiene practices, including wearing shoes in endemic areas and avoiding contact with contaminated soil or feces.
- Provide Education: Nurses play a crucial role in providing education to patients and caregivers about the transmission, symptoms, and treatment of hookworm disease, as well as preventive measures to minimize the risk of reinfection and complications.
- Supportive Care: Nurses provide supportive care to individuals affected by hookworm disease, including nutritional support to address deficiencies caused by chronic blood loss, psychological support to cope with the emotional impact of the disease, and monitoring for complications or adverse effects of treatment.
Environment
- A nurse should make sure there is a clean and hygienic environment to prevent further infection. Maintain a comfortable and quiet atmosphere to promote rest and a quick recovery.
- Make sure to implement infection control measures, such as hand hygiene and environmental sanitation. Then provide adequate ventilation and temperature control to enhance patient comfort.
Observation
- Monitor vital signs regularly to assess for signs of dehydration or infection. Observe for signs of fatigue, weakness, and respiratory distress.
- Monitor stool frequency, consistency, and color to evaluate diarrhea and assess for improvement. Document intake and output to monitor fluid balance and detect signs of dehydration.
Psychological Care
- Provide emotional support to the patient and reassurance to alleviate anxiety and stress. Encourage open communication with the patient and address any concerns or fears the patient may have.
- Give education to the patient about the infection, its treatment, and the importance of adherence to medication and hygiene practices. Collaborate with the healthcare team to address any psychosocial issues or mental health concerns.
Hygiene
- Teach proper hand hygiene techniques to prevent the spread of infection to other patients in the ward. Assist with personal hygiene activities, such as bathing and grooming, as needed.
- Ensure clean and sanitized bedding and clothing to minimize the risk of re-infection. Educate the patient and family members on environmental hygiene practices to reduce exposure to contaminated soil or water.
Exercises
- Encourage light physical activity, such as walking or stretching, to promote circulation and prevent muscle weakness. Provide guidance on breathing exercises to improve lung function and alleviate respiratory symptoms.
- Collaborate with physical therapy for customized exercise programs tailored to the patient’s condition and capabilities. Monitor the patient during exercise sessions and adjust activities as needed based on their tolerance and energy levels.
Nutrition
- Make sure to check the dietary intake and nutritional status to identify deficiencies and develop individualized meal plans. Offer small, frequent meals and snacks to maintain energy levels and support healing.
- Provide education on foods rich in iron, vitamins, and minerals to promote recovery from anemia and enhance immune function. Collaborate with a dietitian to address specific nutritional needs and monitor weight changes.
Elimination
- Monitor bowel habits and provide interventions to manage diarrhea and promote regular bowel movements. Offer dietary modifications, such as increasing fiber intake or avoiding irritating foods, to regulate bowel function.
- Administer prescribed medications, such as antidiarrheals or stool softeners, as ordered by the healthcare provider. Educate the patient on proper toilet hygiene and encourage frequent handwashing to prevent the spread of infection.
Medication
- Administer anthelmintic medications, such as albendazole or mebendazole, as prescribed by the healthcare provider. Monitor for adverse reactions to medications and report any concerns to the healthcare team.
- Educate the patient on the purpose, dosage, and potential side effects of prescribed medications. Ensure compliance with the medication regimen and provide reminders as needed to promote treatment effectiveness.
Advice at Discharge
- Emphasize the importance of completing the full course of prescribed medications to ensure the eradication of the infection. Provide instructions on proper hygiene practices, including handwashing and avoiding contact with contaminated soil.
- Encourage follow-up appointments with healthcare providers for monitoring and assessment of treatment effectiveness. Offer resources and support services, such as community health clinics or support groups, for ongoing care and assistance with managing the infection.
Prevention
Sanitation Practices
- Avoid defecating in open areas, and use designated latrines or toilets to dispose of waste properly.
- Refrain from using human excrement, raw sewage, or untreated “night soil” as fertilizer in agriculture, as these can serve as breeding grounds for hookworm larvae.
Deworming
- Implement regular deworming programs in communities, especially in areas where hookworm infection is prevalent.
- Deworming medications can help eliminate existing infections and prevent re-infections.
Hand Hygiene
- Promote proper handwashing practices, particularly after using the toilet, before preparing or consuming food, and after handling soil or waste.
- Encourage the use of soap and clean water for thorough handwashing, as this helps remove hookworm larvae and prevents transmission.
Footwear Use
- Wear shoes or protective footwear, especially in areas where soil contamination with hookworm larvae is likely, such as sandy or loamy soil.
- Cover feet properly to minimize skin contact with contaminated soil and reduce the risk of larval penetration.
Public health education
- Conduct public health education campaigns to raise awareness about the transmission and prevention of hookworm infections.
- Provide information about the importance of sanitation, hygiene, and deworming in preventing infection and improving community health.
Safe Agricultural Practices
- Educate farmers and agricultural workers about the risks associated with using human waste as fertilizer and promote the use of safer alternatives.
- Encourage the proper composting and treatment of organic waste to eliminate pathogens, including hookworm larvae, before using it in agriculture.
Environmental Management
- Implement measures to improve environmental sanitation, such as proper waste disposal, sewage treatment, and soil management practices.
- Drain stagnant water sources and minimize conditions conducive to the survival and proliferation of hookworm larvae in the environment.
Community Engagement
- Engage community members in efforts to prevent hookworm infection, including participation in deworming campaigns, sanitation improvement initiatives, and hygiene promotion activities.
- Foster community ownership and collaboration to sustain long-term prevention efforts and reduce the burden of hookworm infection in endemic areas.
Complications
- Anemia: Chronic hookworm infection can lead to iron deficiency anemia due to the loss of blood caused by the parasites feeding on the host’s intestinal mucosa.
- Malnutrition: Prolonged hookworm infection can result in malabsorption of nutrients, leading to protein-energy malnutrition and deficiencies in essential vitamins and minerals.
- Growth Retardation: Children with chronic hookworm infection may experience stunted growth and delayed development due to the nutritional deficiencies and chronic inflammation associated with the infection.
- Cognitive Impairment: Severe hookworm infection, particularly in children, can impair cognitive function and intellectual development, leading to learning difficulties and poor academic performance.
- Intestinal Complications: Inflammatory reactions in the intestines caused by hookworms can result in symptoms such as abdominal pain, diarrhea, and gastrointestinal bleeding.
- Respiratory Symptoms: Migration of hookworm larvae through the lungs can cause respiratory symptoms such as cough, wheezing, and shortness of breath.
- Skin Disorders: Ground itch, a common symptom of hookworm infection, can lead to dermatitis, itching, and skin irritation at the site of larval penetration.
- Secondary Infections: A persistent hookworm infection can weaken the immune system, increasing the risk of secondary bacterial, fungal, or parasitic infections.
- Pregnancy Complications: Hookworm infection during pregnancy can lead to complications such as intrauterine growth restriction, preterm birth, and low birth weight in newborns.
- Cardiovascular Effects: Severe anemia resulting from hookworm infection can strain the cardiovascular system, leading to symptoms such as palpitations, fainting, and chest pain.
- Mental Health Issues: Chronic illness and its associated symptoms can have psychological effects, including depression, anxiety, and reduced quality of life.
- Fatalities: Although rare, severe complications of hookworm infection, such as massive gastrointestinal bleeding or severe anemia, can lead to fatalities if left untreated.
Read more: Medical-Surgical Nursing
Read more: Tapeworms | Causes | Signs and symptoms | Treatment | Nursing Management
[…] Read more: Hook Worm Disease | Causes | Pathophysiology | Signs and Symptoms | Treatment | Nursing Management […]