Introduction
Abortion, the deliberate termination of a pregnancy, is a multifaceted and often emotionally charged topic that intersects with diverse aspects of human life medical, ethical, legal, and social. Whether spontaneous or induced, abortion evokes discussions on women’s reproductive rights, healthcare accessibility, and the complex interplay of personal choices and societal values. As we explore this intricate subject, it is crucial to approach it with sensitivity and respect for the diverse perspectives that surround it, acknowledging the profound impact it has on individuals, families, and societies.
Definition
Abortion is the intentional termination of a pregnancy, resulting in the removal or expulsion of the embryo or fetus from the uterus (Chinyama, 2022). This process can occur spontaneously, known as a miscarriage, or it can be induced through medical or surgical procedures. Induced abortion is a deliberate decision made by a woman or a couple for various reasons, including health concerns, fetal abnormalities, or personal circumstances.
The topic of abortion is complex and often involves ethical, legal, and societal considerations, with debates surrounding women’s reproductive rights, the status of the fetus, and access to safe and legal healthcare services. Abortion methods can include medical procedures using medications or surgical interventions, and the legal and cultural perspectives on abortion vary widely around the world.
Abortion of Pathophysiology
The pathophysiology of abortion, whether spontaneous (miscarriage) or induced, involves complex processes at the molecular, cellular, and tissue levels. Understanding these mechanisms is crucial for healthcare professionals in diagnosing, managing, and providing appropriate care to individuals experiencing abortion. Here, we’ll explore the pathophysiology of both spontaneous and induced abortions:
-
Spontaneous Abortion (Miscarriage)
Genetic Abnormalities: Chromosomal abnormalities in the developing embryo are a leading cause of spontaneous abortion. Errors during fertilization or early cell division can result in a nonviable embryo, prompting the body to terminate the pregnancy.
Hormonal Imbalances: Disruptions in the delicate balance of hormones essential for maintaining pregnancy, such as progesterone, can contribute to miscarriage. Inadequate hormonal support may lead to the failure of implantation or the inability to sustain early pregnancy.
Uterine Abnormalities: Structural issues with the uterus, such as abnormalities in shape or the presence of fibroids, may interfere with implantation or contribute to the expulsion of the embryo.
Maternal Health Conditions: Conditions like diabetes, thyroid disorders, autoimmune diseases, or infections can increase the risk of miscarriage.
Immunologic Factors: Immune system reactions, where the body perceives the developing embryo as a threat, can lead to rejection and spontaneous abortion.
-
Induced Abortion
Medical Abortion
Mifepristone and Misoprostol: Mifepristone, an anti-progestin, blocks progesterone receptors, leading to the breakdown of the uterine lining. Misoprostol induces uterine contractions, facilitating the expulsion of the gestational sac.
Methotrexate: Interferes with cell division and inhibits the growth of the embryo.
Surgical Abortion
Suction Aspiration: A vacuum aspiration procedure removes the contents of the uterus, including the embryo or fetus.
Dilation and Curettage (D&C): Involves dilating the cervix and scraping or suctioning the uterine lining to remove the embryo or fetal tissues.
Dilation and Evacuation (D&E): Similar to D&C but performed later in pregnancy, usually between 13 to 24 weeks.
Hormonal Methods: High doses of certain hormones, such as prostaglandins or oxytocin, can stimulate uterine contractions, leading to the expulsion of the pregnancy.
Common Pathophysiological Events
Decidual Breakdown: The decidual layer, which lines the uterus and supports the pregnancy, undergoes breakdown in response to hormonal changes or medical interventions.
Uterine Contractions: Uterine contractions are a common feature in both spontaneous and induced abortions, facilitating the expulsion of the pregnancy.
Inflammatory Response: The body often initiates an inflammatory response as part of the natural healing process, particularly in spontaneous abortions.
Cervical Changes: The cervix undergoes changes to allow the passage of pregnancy-related tissues during abortion.
Understanding the pathophysiology of abortion enables healthcare professionals to provide empathetic and informed care to individuals experiencing this reproductive event. It also aids in identifying potential risk factors, ensuring appropriate counseling, and guiding future reproductive health decisions.
POTENTIAL RISK FACTORS
Risk factors are conditions or characteristics that increase the likelihood of an individual developing a particular disease or experiencing a specific health-related event. In the context of abortion, whether spontaneous (miscarriage) or induced, various factors can contribute to an increased risk. Understanding these risk factors is crucial for healthcare providers in offering personalized care, counseling, and preventive measures. Here are some key risk factors associated with abortion:
-
Age
Spontaneous Abortion: Advanced maternal age, typically defined as 35 years and older, is associated with an increased risk of chromosomal abnormalities in the developing embryo, leading to spontaneous abortion.
Induced Abortion: Teenagers may face unique social and emotional challenges, impacting their reproductive health decisions.
-
Previous Pregnancy History
Spontaneous Abortion: Women who have a history of previous miscarriages may be at a higher risk for subsequent spontaneous abortions.
Induced Abortion: A history of prior induced abortions may impact subsequent reproductive outcomes.
-
Genetic Factors
Spontaneous Abortion: Genetic abnormalities in the developing embryo can increase the risk of spontaneous abortion.
Induced Abortion: Genetic testing may identify fetal abnormalities, influencing the decision for an induced abortion.
-
Uterine Abnormalities
Spontaneous Abortion: Structural issues with the uterus, such as fibroids or abnormalities in shape, may contribute to spontaneous abortion.
Induced Abortion: Uterine abnormalities can affect the success of certain abortion procedures.
-
Chronic Medical Conditions
Spontaneous Abortion: Conditions like diabetes, thyroid disorders, autoimmune diseases, and hypertension can increase the risk of spontaneous abortion.
Induced Abortion: Some medical conditions may influence the choice for induced abortion due to potential health risks.
-
Infections
Spontaneous Abortion: Certain infections, especially those affecting the reproductive organs, can increase the risk of spontaneous abortion.
Induced Abortion: Infections can pose risks during and after abortion procedures.
-
Lifestyle Factors
Spontaneous Abortion: Smoking, excessive alcohol consumption, and illicit drug use can contribute to an increased risk of spontaneous abortion.
Induced Abortion: Lifestyle factors may influence reproductive health decisions, including the choice for induced abortion.
-
Emotional and Psychosocial Factors
Spontaneous Abortion: High levels of stress or emotional trauma may be associated with an increased risk of spontaneous abortion.
Induced Abortion: Emotional well-being and support are crucial considerations for those opting for induced abortion.
-
Access to Healthcare
Spontaneous Abortion: Limited access to prenatal care may impact the identification and management of risk factors associated with spontaneous abortion.
Induced Abortion: Access to safe and legal abortion services is essential for minimizing risks associated with induced abortion.
Identifying and addressing these risk factors in a holistic manner is essential for providing comprehensive reproductive healthcare, offering appropriate counseling, and supporting individuals in their reproductive decisions. It is important to note that individual circumstances vary, and healthcare providers consider a personalized approach based on the unique needs and characteristics of each individual.
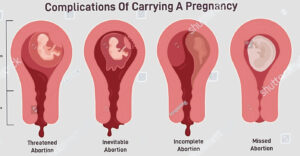
TYPES OF ABORTION
Abortion, the intentional termination of a pregnancy, can occur through various methods, each with its own characteristics and considerations. The two main types of abortion are spontaneous (miscarriage) and induced. Induced abortions can further be categorized into medical and surgical methods. Here’s an overview of the types of abortion:
-
Spontaneous Abortion (Miscarriage)
Definition: Unintentional termination of a pregnancy before the 20th week.
Causes: Often due to genetic abnormalities, hormonal imbalances, uterine abnormalities, or maternal health conditions.
Characteristics: Typically occurs naturally without medical intervention.
-
Induced Abortion
Definition: Deliberate termination of a pregnancy through medical or surgical means.
-
Medical Abortion
Methods
Mifepristone and Misoprostol: Mifepristone, an anti-progestin, blocks progesterone receptors, leading to the breakdown of the uterine lining. Misoprostol induces uterine contractions, facilitating the expulsion of the gestational sac.
Methotrexate: Interferes with cell division and inhibits the growth of the embryo.
Timing: Typically used during the early stages of pregnancy, up to the first 10 weeks.
Characteristics: Does not require surgery; often preferred for its non-invasive nature.
-
Surgical Abortion
Methods
Suction Aspiration: A vacuum aspiration procedure that removes the contents of the uterus, including the embryo or fetus.
Dilation and Curettage (D&C): Involves dilating the cervix and scraping or suctioning the uterine lining to remove the embryo or fetal tissues.
Dilation and Evacuation (D&E): Similar to D&C but performed later in pregnancy, usually between 13 to 24 weeks.
Timing: Surgical methods are typically used later in the first trimester or during the second trimester.
Characteristics: Involves a surgical procedure, usually conducted in a healthcare facility.
-
Aspiration Abortion
Method: Similar to suction aspiration, it involves using suction to remove the contents of the uterus. Commonly used in the first trimester.
Characteristics: A less invasive surgical method.
-
Induction Abortion
Method: Involves inducing labor through medications, leading to the expulsion of the fetus. Typically performed later in the second trimester.
Characteristics: Mimics a natural childbirth process.
-
Intrauterine Instillation
Method: Involves injecting a solution, such as saline or prostaglandin, into the uterus to induce contractions and terminate the pregnancy. Historically used but less common today.
Characteristics: Considered outdated due to associate risks.
Each type of abortion has its own set of considerations, risks, and appropriate contexts. The choice of method often depends on factors such as gestational age, individual health considerations, and personal preferences. Access to safe and legal abortion services is essential to ensure the well-being of individuals seeking abortion and to minimize associated risks.
SIGNS AND SYMPTOMS
Signs and symptoms associated with abortion can vary depending on whether it is spontaneous (miscarriage) or induced. Here are the common signs and symptoms for each:
-
Spontaneous Abortion (Miscarriage)
Vaginal Bleeding: One of the earliest signs is often vaginal bleeding, which may range from light spotting to heavy bleeding.
Abdominal Pain: Cramping or abdominal pain, similar to menstrual cramps, may accompany the bleeding.
Tissue Passing: In some cases, there may be the passage of tissue or clots from the vagina.
Back Pain: Pain or discomfort in the lower back can occur.
Loss of Pregnancy Symptoms: If the miscarriage is progressing, there may be a sudden decrease or loss of pregnancy symptoms such as breast tenderness and nausea.
Fluid Discharge: Clear or pinkish fluid discharge from the vagina may be noticed.
Fever and Chills: In some cases, a fever and chills may occur, especially if there is an infection.
-
Induced Abortion
Vaginal Bleeding: Bleeding is a common sign, and the amount can vary depending on the method used.
Abdominal Pain or Cramping: Similar to spontaneous abortion, induced abortion may be accompanied by abdominal pain or cramping.
Nausea and Vomiting: Some individuals may experience nausea and vomiting, especially with medical abortion methods.
Fatigue: Feeling tired or fatigued can be a common symptom.
Dizziness: Dizziness or lightheadedness may occur, particularly during and after the procedure.
Changes in Vaginal Discharge: Changes in vaginal discharge, including the passage of tissue, may be observed.
Emotional Response: Emotional reactions such as relief, sadness, or a mix of emotions can be expected.
It’s important to note that signs and symptoms can vary widely among individuals, and not everyone may experience the same set of manifestations.
In Addition, these symptoms can be influenced by factors such as gestational age, the method of abortion, and individual health conditions. If someone is experiencing symptoms related to abortion, it is crucial to seek prompt medical attention for appropriate evaluation and care. Access to supportive healthcare services is vital to address both the physical and emotional aspects of the abortion process.
DIAGNOSTIC TESTS
Diagnostic tests related to abortion are conducted to assess the status of the pregnancy, confirm the occurrence of an abortion, and evaluate the well-being of the individual. The specific tests performed can vary depending on whether the abortion is spontaneous (miscarriage) or induced. Here are some common diagnostic tests associated with abortion:
-
Ultrasound
Purpose: To visualize the uterus and assess the status of the pregnancy.
Application: Can confirm the presence of a gestational sac, fetal heartbeat, and evaluate the overall health of the pregnancy.
Usage: Used in both spontaneous and induced abortion scenarios.
-
Blood Tests
Purpose: To measure specific hormones related to pregnancy.
Beta-hCG Levels: Serial measurements of beta-human chorionic gonadotropin (hCG) levels can help determine the viability of the pregnancy and whether it is progressing as expected. A decline in beta-hCG levels may indicate a nonviable pregnancy or the completion of an abortion.
-
Pelvic Exam
Purpose: To assess the condition of the cervix and vagina.
Application: Can help determine if the cervix has dilated and if any tissue or clots are present.
-
Hysteroscopy
Purpose: To visually examine the inside of the uterus.
Application: A thin, lighted tube (hysteroscope) is inserted through the cervix to view the uterine lining, helping identify any retained tissue.
-
Complete Blood Count (CBC)
Purpose: To assess overall blood health.
Application: Anemia or infection can be detected through CBC, especially in cases of heavy bleeding or infection following abortion.
-
Tissue Examination
Purpose: To analyze tissues passed during abortion.
Application: Tissue examination can provide insights into the cause of a spontaneous abortion, especially if genetic abnormalities or other issues are suspected.
-
Rh Factor Testing
Purpose: To determine the Rh status of the individual.
Application: Rh factor testing is essential, especially if the individual is Rh-negative and there is a risk of Rh incompatibility with the fetus.
These diagnostic tests are crucial in determining the status of a pregnancy, confirming the occurrence of an abortion, and identifying any potential complications or underlying factors. The choice of tests may vary based on the clinical scenario, gestational age, and individual health considerations. Access to timely and appropriate diagnostic procedures is essential for providing comprehensive care and support to individuals experiencing abortion.
MEDICAL MANAGEMENT
Medical management in the context of abortion involves the use of medications and supportive care to either induce abortion or manage the consequences of a spontaneous abortion (miscarriage). The approach may differ based on whether the abortion is spontaneous or induced. Here is an overview of medical management strategies:
-
Medical Abortion (Induced)
Method: Involves the use of medications to terminate a pregnancy.
Common Medications
Mifepristone: An anti-progestin that blocks progesterone receptors, leading to the breakdown of the uterine lining.
Misoprostol: A prostaglandin that induces uterine contractions, facilitating the expulsion of the gestational sac.
Administration: Mifepristone is typically taken first, followed by misoprostol within a specified timeframe.
Timing: Effective for early pregnancies, usually up to the first 10 weeks.
Supervision: Often done under medical supervision, with follow-up visits to confirm the completion of the abortion.
Efficacy: High success rates when administered appropriately, with effectiveness exceeding 95%.
-
Supportive Care for Spontaneous Abortion (Miscarriage)
Monitoring: Close monitoring of symptoms, such as bleeding and cramping, to assess the progression of the miscarriage.
Pain Management: Analgesics may be prescribed to manage pain and discomfort associated with cramping.
Anti-D Immunoglobulin (RhoGAM): Administered in cases of Rh-negative individuals to prevent Rh sensitization if there is any potential mixing of maternal and fetal blood.
Emotional Support: Counseling and emotional support to address the psychological impact of miscarriage.
Follow-up Care: Follow-up appointments to ensure the complete expulsion of pregnancy-related tissues and assess the individual’s physical and emotional well-being.
-
Treatment of Complications
Infection Management: Antibiotics may be prescribed to manage or prevent infections, especially in cases of incomplete abortion.
Hemorrhage Control: In cases of heavy bleeding, medical interventions may be needed to control hemorrhage.
-
Rh Incompatibility Management
Anti-D Immunoglobulin (RhoGAM): Administered if the individual is Rh-negative and there is a risk of Rh incompatibility with the fetus.
-
Follow-up Care
Post-Abortion Counseling: Counseling and support services to address the emotional and psychological aspects of abortion.
Contraceptive Counseling: Discussion about contraception and family planning options for the future.
Medical management aims to ensure the safe and effective completion of the abortion process while addressing any complications or consequences. Close collaboration with healthcare providers and access to supportive care are integral components of medical management in abortion scenarios, promoting the overall well-being of individuals undergoing the process.
SURGICAL MANAGEMENT
Surgical management of abortion involves procedures that are performed to either terminate a pregnancy or address complications arising from a spontaneous abortion (miscarriage). The choice of surgical method depends on factors such as gestational age, individual health, and clinical considerations. Here are common surgical management approaches:
-
Suction Aspiration
Procedure: A suction or vacuum aspiration procedure to remove the contents of the uterus, including the gestational sac.
Timing: Typically used during the early stages of pregnancy, within the first 6 to 16 weeks.
Process: The cervix is dilated, and a suction device is used to gently remove the uterine contents.
-
Dilation and Curettage (D&C)
Procedure: Involves dilating the cervix and using a curette (a spoon-shaped instrument) to scrape and remove the uterine lining.
Timing: Commonly performed during the first trimester.
Process: The cervix is dilated, and the curette is used to carefully remove tissues from the uterus.
-
Dilation and Evacuation (D&E)
Procedure: Similar to D&C but performed later in pregnancy, usually between 13 to 24 weeks.
Timing: Common for second-trimester induced abortions.
Process: The cervix is dilated, and forceps are used to remove the fetus and other pregnancy-related tissues.
-
Hysteroscopy
Procedure: Involves the insertion of a thin, lighted tube (hysteroscope) through the cervix to visually examine the inside of the uterus.
Timing: Used to assess and manage complications such as retained tissue.
-
Laparoscopy
Procedure: A minimally invasive surgical procedure involving the insertion of a thin tube with a camera (laparoscope) through small incisions in the abdomen.
Timing: May be used to address specific complications or assess pelvic organs.
-
Laparotomy
Procedure: A more invasive surgical procedure involving a larger abdominal incision.
Timing: Reserved for cases with severe complications or in the presence of specific medical conditions.
-
Cerclage Removal
Procedure: Removal of a cervical cerclage (stitch) that may have been placed earlier during pregnancy.
Timing: Performed in cases where a cerclage is contributing to complications.
-
Treatment of Complications
Infection Management: Antibiotics may be prescribed to manage or prevent infections.
-
Rh Incompatibility Management
Anti-D Immunoglobulin (RhoGAM): Administered if the individual is Rh-negative to prevent Rh sensitization.
Surgical management is often conducted in a healthcare facility, and the choice of procedure depends on various factors, including gestational age, medical history, and the specific circumstances surrounding the abortion. Access to skilled healthcare professionals and appropriate facilities is crucial to ensure the safety and effectiveness of surgical management in abortion cases.
NURSING MANAGEMENT
Nursing management in the context of abortion involves the comprehensive care and support provided by nurses to individuals undergoing either spontaneous (miscarriage) or induced abortion. This encompasses a range of responsibilities, including emotional support, monitoring physical well-being, and educating individuals about the abortion process and post-procedural care. Here are key aspects of nursing management in abortion scenarios:
-
Assessment
Physical Assessment: Conduct a thorough physical assessment to evaluate the individual’s overall health, including vital signs, abdominal pain, bleeding, and any signs of infection.
Emotional Assessment: Assess emotional well-being, offering a safe space for individuals to express their feelings and concerns related to the abortion.
-
Emotional Support
Counseling: Provide counseling and emotional support throughout the abortion process, addressing any fears, anxieties, or emotional reactions. Acknowledge and validate the individual’s emotions.
-
Education
Abortion Process: Educate individuals about the chosen abortion method, potential side effects, and what to expect during and after the procedure.
Post-Abortion Care: Provide clear instructions on post-procedural care, including signs of complications, when to seek medical attention, and contraceptive options.
-
Pain Management
Assessment: Assess and manage pain associated with the abortion process, providing appropriate analgesics as needed. Educate individuals about pain management options.
-
Monitoring
Vital Signs: Regularly monitor vital signs to detect any signs of complications, such as infection or excessive bleeding.
Bleeding and Discharge: Monitor the amount and type of bleeding, as well as any abnormal discharge.
Signs of Infection: Be vigilant for signs of infection, such as fever, chills, or abdominal tenderness.
-
Infection Prevention
Hygiene Education: Educate individuals on proper hygiene practices to prevent infections, especially after surgical procedures. Emphasize the importance of handwashing.
-
Rh Incompatibility Management
Anti-D Immunoglobulin (RhoGAM): Administer RhoGAM to Rh-negative individuals as needed to prevent Rh sensitization.
-
Contraceptive Counseling
Family Planning: Provide information and counseling on contraceptive options to help individuals make informed decisions about future family planning.
-
Referral and Follow-up
Referral to Support Services: Facilitate referrals to mental health professionals or support groups, especially for those experiencing emotional distress.
Follow-up Care: Arrange for follow-up appointments to monitor the individual’s physical and emotional recovery.
-
Advocacy
Patient Rights: Advocate for individuals’ rights to access safe and compassionate reproductive healthcare. Ensure that individuals are informed about their choices and have the necessary support.
Nursing management plays a critical role in providing holistic care, addressing the physical and emotional needs of individuals undergoing abortion. Compassion, empathy, and clear communication are essential components of nursing care in these sensitive situations.
Conclusion
In conclusion, the discourse surrounding abortion is a nuanced one, encompassing a spectrum of beliefs, values, and ethical considerations. The decision to terminate a pregnancy, whether for medical, personal, or socioeconomic reasons, is deeply personal, and its implications are far-reaching. As we navigate conversations about abortion, it is essential to foster open dialogue, prioritize women’s health and autonomy, and work towards comprehensive reproductive healthcare that addresses the complexities inherent in this sensitive and crucial aspect of human experience.
Read more about: Menstrual Cycle
Read more about: Breastfeeding